Photo source: World Heart Foundation
Adeniyi used to think hypertension was something that happened to “other people”, especially older people or stressed-out people. Then one day, his uncle, who was full of life at 45, had a minor stroke. The culprit? Undiagnosed high blood pressure. He never saw it coming. He thought he was fit and very healthy until this incident. He is not alone.
“I didn’t know until it was serious.” That’s a common story. Many people are walking around unaware that they are one unchecked blood pressure reading away from a life‑changing incident.
They call it the silent killer for a reason. You could have it and never feel a thing until a stroke, heart attack, or kidney disease changes everything. It is hard to detect because it does not always cause symptoms. The only way to know is to get your blood pressure checked. Hypertension, also referred to as high blood pressure, is more than a personal health issue; it is a global epidemic that remains one of the world’s top contributors to death yearly.
While we have more tools than ever, from AI-driven wearables to personalized nutrition, the Black community globally continues to bear a disproportionate burden of this silent killer. Whether you are in Philadelphia, Lagos, or London, the numbers tell a story that requires our urgent attention.
A global look at the occurrence of hypertension
Hypertension is when the pressure in your blood vessels is too high (140/90 mmHg or higher). While the number of people with high blood pressure has continued to rise, control rates remain low in many countries, and the burden still falls disproportionately on Black communities, according to global and national reports.
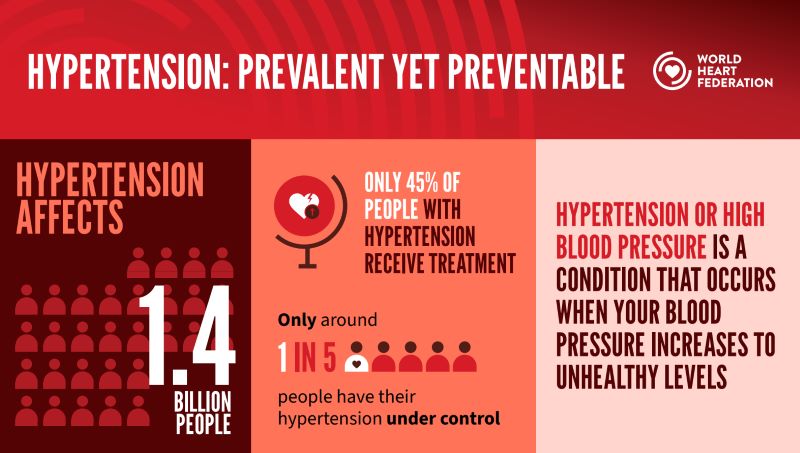
The second global hypertension report by the World Health Organization (WHO), released in 2025, shows that an estimated 1.4 billion adults aged 30-79 lived with hypertension in 2024, yet just over one in five have the condition adequately controlled either through medication or addressing modifiable health risks. This represents 33% of the population in this age range, and has changed little since 1990, when prevalence was 32%.
Analysis of data from 195 countries and territories shows that 99 of them have national hypertension control rates below 20%.
As WHO Director-General, Dr Tedros Adhanom Ghebreyesus warned in the report, “Every hour, over 1000 lives are lost to strokes and heart attacks from high blood pressure, and most of these deaths are preventable.”
The irony is that hypertension is easily detectable by measuring blood pressure, at home or in a healthcare facility. It is also often effectively treated with medications.
Analysis of data from 195 countries and territories shows that 99 of them have national hypertension control rates below 20%. The majority of those affected live in low and middle-income countries, where health systems face significant resource constraints. So while the rate of hypertension has decreased in wealthy countries, it has increased in many low or middle-income countries.
Countries such as Canada, Costa Rica, Iceland, and the Republic of Korea have achieved hypertension control rates >50%. Not much has changed since 2019, when some of the highest rates were seen in countries such as the Dominican Republic, Jamaica, and Paraguay, among others.
Photo source: World Health Organization
In the United States, the disparity persists. Black adults continue to have a higher prevalence and lower control of hypertension. The rate of high blood pressure among Black adults in the United States is among the highest in the world.
In true FunTimes fashion, this ought to be explored somewhat. Why are Black people experiencing an increase in hypertension?
Hypertension and Black populations
The National Health Fund in Jamaica states that the occurrence of high blood pressure is particularly common in Black middle-aged and elderly people. Most health organizations share similar sentiments. Among the more plausible causes are genetic and environmental factors.
Though Black people worldwide have rates of high blood pressure that are similar to those of white people, in the US, there is a dramatic difference. According to reports from the American Heart Association (AHA), more than 55% of Black adults in the United States have hypertension. Also, the mortality in Black Americans is double that of White Americans.
As for the use of hypertension-based medication, the AHA states that the lack of access to medication and distrust of health care professionals based on historical discrimination are among the contributing factors to lower adherence to blood pressure medications.
Also, experts think that social and economic factors, including discrimination and economic inequality, are responsible for this difference in the US.
In Africa, diagnosis, care, and control of hypertension are constrained by low awareness about the condition, limited access to health services, overburdened health systems, health workforce challenges, lack of access to affordable medicines, and non-compliance with drug regimens. Rising obesity rates, unhealthy lifestyles, and insufficient patient education compound the threat.
So, not only are there external factors adding to the issue, but there are also internal issues that exacerbate the problem of the increased incidence of hypertension among Black people.
Hypertension risk factors
Some of the risk factors for hypertension are generally classified as modifiable and non-modifiable. The non-modifiable risk factors are things you cannot change. They include a familial history of hypertension, having co-existing diseases such as diabetes and kidney disease, and generally being over the age of 65. The modifiable risk factors are those you can change. These can be addressed to reduce the chances of hypertension. They include physical inactivity, unhealthy diets, overconsumption of alcohol, and smoking.
The lack of physical activity plays a crucial role. Exercise is beneficial to the body externally and internally. Though a decrease in activity can lead to many issues, it should not be ruled out as a factor in the development of hypertension.
The unhealthy diets mentioned include those high in saturated and trans fats and in sodium. Not to rub salt in wounds, but the “additional flavor” you add to your meals with various seasoning shakers to add the right taste often includes salt. This leads to excessive salt intake over time. Something you might not know is that sodium can be hidden in other foods you eat. So, over time, this also contributes to excessive salt intake.
Addressing the salt issue
Salt is used as a universal flavor improver, hence the propensity to indulge in excessive salt consumption! However, high salt intake has been shown to be associated with high blood pressure, especially in blacks.
Dr Ramon Moronkola, Consultant Interventional Cardiologist at LASUTH, sheds more light on the issue.
“Salt contains sodium, and sodium plays a major role in regulating the body’s fluid balance. When people consume too much salt, the body retains more water in the bloodstream. This increases the volume of blood circulating through the vessels, raising blood pressure.
“Over time, persistent high salt intake can also stiffen blood vessels and impair the normal function of the kidneys, both of which contribute to hypertension.”

Photo source: LinkedIn / Ramon Moronkola
Why is salt such a big problem for Black communities?
The key concept here is salt sensitivity, the degree to which a person’s blood pressure rises in response to eating salt. Research shows that Black populations are more salt-sensitive than White populations. This means when Black individuals consume salt, their bodies retain more sodium.
“Another important point is that many people are “salt sensitive.” In these individuals, blood pressure rises significantly when they consume a high-salt diet. This is particularly common among people of African descent, older adults, and individuals with kidney disease or diabetes.
“Because hypertension is a leading risk factor for stroke, heart failure, kidney disease, and heart attacks, reducing salt intake is one of the most effective lifestyle strategies for prevention and control.
“The World Health Organization (WHO) recommends that adults consume less than 5 grams of salt per day, which is roughly one teaspoon. Unfortunately, many people consume two to three times this amount, often without realizing it. A large portion of salt intake actually comes from processed foods, packaged snacks, seasoning cubes, fast foods, and restaurant meals, not just from the salt shaker,” Dr Moronkola says.
He suggested healthier ways to flavor food while reducing salt intake. They include:
- Natural herbs: basil, thyme, rosemary, parsley
- Spices: garlic, ginger, turmeric, black pepper, paprika
- Citrus flavors: lemon or lime juice
- Onions and fresh peppers
According to him, these alternatives enhance flavor without increasing blood pressure risk, and gradually reducing salt intake also allows the taste buds to adapt, making lower-salt food more acceptable over time.
When asked at what age people should start checking their blood pressure regularly, he suggests starting screening in early adulthood, around age 18.
“Even though hypertension becomes more common with age, it is increasingly being diagnosed in younger adults. For most healthy adults, at least once every year is reasonable if previous readings are normal. However, people with risk factors should check their blood pressure more frequently. These risk factors include family history of hypertension, overweight or obesity, diabetes, kidney disease, high salt intake, and a sedentary lifestyle.
“One challenge with hypertension is that it is often called the “silent killer” because many people feel completely well until complications like stroke or heart disease occur. Regular blood pressure checks allow for early detection and early treatment, which can prevent these complications.”
The message is clear: reducing sodium intake is important for everyone, but more for Black communities. The 2026 World Health Day theme, Together for Health: Stand with Science, calls on governments, communities, and individuals to act. But as many in the Black community have long pointed out, science and the healthcare system must also stand for them.
What can we do in the meantime?
Know your numbers. Get your blood pressure checked regularly at home, a pharmacy, or a clinic. Reduce your salt intake, cut back on processed foods, stay active, manage stress, limit alcohol, and stop smoking if you do. If you are diagnosed with hypertension, follow your treatment plan and keep your appointments. These steps cannot replace systemic reform, but they can save your life while we push for the change that is needed.



